

Diaphragmatic endometriosis will cause cyclically upper abdominal pain, sometimes pain on inspiration and also referred pain to the shoulders.

Endometriosis involving the bladder is often misdiagnosed as a urinary tract infection for years

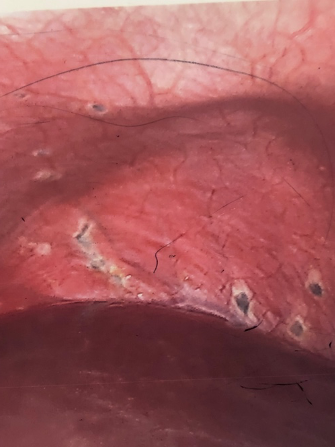
In this patient, there is white scarring on the right uterosacral ligament (middle of picture). The ovary and fallopian tube are to the right. However, early endometriosis also involves the right rectum. She had been misdiagnosed as irritable bowel for years.

This 28 year old woman presented with a history of many years of painful defecation at period time. If the diagnosis had been further delayed, she would have needed a bowel resection. I excised the diseased area by stripping off the peritoneum, and inserted a mirena, and also put her on a course of Zoladex. She has since had two children.

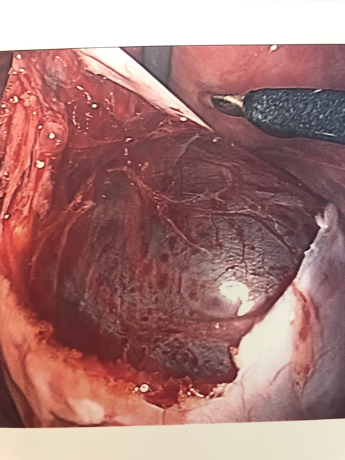
Here, the left ovary is enlarged by an endometrioma, and is stuck to the left posterior surface of the uterus. The left tube is dilated and blocked. The smaller right ovary is stuck to the back of the uterus. She presented with a history of deep pain with intercourse and infertility .
Endometriosis has different appearances and may look different in every single patient .Sure there can be dark ,or black blood, but it can also look brown, red ,white or clear. Areas of scar tissue should also be excised, because they often also contain endometriosis.

To dissect endometriotic disease from the Pouch of Douglas, it is often necessary to dissect out the ureter, starting high up in the pelvis, where normal tissue exists.


In this picture you can see endometriosis mainly on the left uterosacral ligament, but close to the rectum.

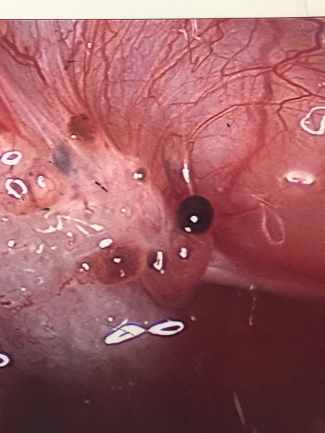
There are numerous areas of endometriosis over the diseased peritoneum, but note the inflammation with bright red blood vessels coursing out from the classic dark lesions..

This endometriosis has been here for some time. There are small pink blisters, larger black areas, but also white areas representing scarring.

Sometimes endometriotic scaring obscures the view of the ureter altogether and a ureteric catheter must be placed from below to identify the position of the ureter in the pelvis, so that dissection of endometriosis can occur safely. This picture shows the ureteric orifice in the bladder.

The ureteric catheter is fed up through a telescope called a cystoscope, to the level of the pelvic brim.


Laparoscopic Division of Adhesions
If a patient has had a previous mid-line incision, usually for bowel surgery or trauma, the safest point of entry for the laparoscope is in the mid-clavicular line underneath the ribcage. A small telescope can be inserted through that incision and looks immediately towards the umbilicus. If there are not adhesions under the umbilicus, of course we can put a larger telescope in if necessary. The pictures adjacent show various patients with different types of adhesions present and how they are divided.

A large right ovarian mass (cyst), is seen behind the uterus which is being held forward with a probe.

A small left sided fimbrial cyst coming from the fimbrial end of the tube. Note that the stalk is twisting ,and if it continues to twist ,it will twist off its own blood supply. If this happens the patient will suffer severe pain, often associated with vomiting. Similar pain is associated with the twisting of an ovary (and a testicle in the case of a male).Such pain begins in the region of the kidney, is colicky in nature ,and radiates down towards the pelvis. The reason the pain begins in the kidney region, is that this is where the ovary develops in the embryo.

A left ovarian teratoma,(also called a dermoid cyst)These unusual cysts are more often benign, but can be malignant with increasing age. They are the most common pathological cysts in young women.
A large benign simple cyst, is here being shelled out from the left ovary. I take washings from the pelvis by first irrigating the pelvis in the region of the ovarian cyst, then sucking it back out into a container. The fluid is sent to the pathologist and examined under a microscope.

A large right sided para-ovarian cyst, before removal. These cysts do not actually involve the ovary itself, but can cause pressure symptoms. They can also be misdiagnosed as ovarian cysts when looked at by ultrasound.

A cyst-adenoma (a benign cyst),is here being shelled out from the ovary .As with any other suspicious looking ovarian cyst, peritoneal washings are taken here too, and sent for analysis .

An ovarian endometrioma. First the outer capsule is incised.

Then the old blood (the fluid that has a chocolate appearance), is drained out.

Finally here, the inner capsule is in the process of being shelled out. If this is not done, the endometrioma will simply reform.

A normal corpus luteum cyst.
These cysts can be 6 cm in diameter, cause severe pain, and because they are associated with increased and prolonged progesterone production, are associated with a delay in menstruation, (with a negative pregnancy test)
To remove the mass (after cancer had already been excluded by using a scan, doing a blood test and visualizing it), the mass is mobilized.
Peritoneal washings are taken off by washing the surface of the ovarian cyst to wash away any potentially malignant cells. These are sent off for cytology to the Lab. Obviously the uterus and the ovarian vessels need to be identified and the ovarian vessels are cauterized.

This picture shows typical” violin string adhesions”, under the diaphragm (it is called Fitzu -Curtis syndrome, after the two Canadian medical students that named them,) and they are caused by Chlamydia infection.

This patient came with symptoms of infertility, and the tubes were seen to be dilated on ultrasound scan. It was obvious the patient would need to have IVF treatment. However, even before IVF the tubes need to be removed because the tubes are filled with embryo toxic fluid and if the tubes are retained, they will drain embryo toxic- fluid into the uterus ,where the embryo is trying to implant.
The pregnancy rate is reduced by 50% if the tubes are retained.

A 3cm submucous fibroid these fibroids protrude into the cavity of the uterus and are associated with very heavy periods

A submucous fibroid that has been partly resected hysteroscopically

490 gram fibroid being removed

490 gram fibroid being removed



