
Uterine Fibroids
/Uterine fibroids or leiomyomata, are one of the most common medical conditions affecting women.
At the age of 40, 40% of women have fibroids – a benign growth of the uterus.



The uterus is a large expulsive muscular organ made of smooth muscle. Its primary role is to contract during labour, but it also contracts during menstruation, often causing period cramps. Fibroids, which are tumors of the uterus, often evoke fear – but they are simply benign lumps or new growths originating from a single cell in the uterine muscle which then begins to grow rapidly.
Almost all uterine fibroids, less than the size of a 20 week pregnancy, are benign (not cancerous). Most fibroids are very small (less than the size of a golf ball) but they can grow to the size of a watermelon. Similarly some women have only one small fibroid while others have dozens of them.
Furthermore, fibroids can also occupy various positions within the uterus. Not all fibroids need to be treated!
It is possible for women to have fibroids and never know it. In some cases they may cause horrendous flooding periods or pressure on the bowel and the bladder. The bigger the fibroids become, the more symptoms the patient has.
A fibroid within the uterine cavity (submucous), may distort the endometrium, or lining of the uterus and cause heavy bleeding.
If a fibroid grows outwards from the side of the uterus, it may block ureters, linking tubes, put pressure on the kidney and indeed put pressure on the bladder. The blockage of urine may cause kidney infections or even kidney damage in severe cases.
Larger fibroids can cause heavy painful periods and irregular bleeding between periods (these are usually submucous or within the uterine cavity. (these are usually submucous or within the uterine cavity). Often they are on a stalk – fibroids on a stalk are easily removed without recourse to hysterectomy, with the use of an operating hysteroscope.
Loss or urine, pain with intercourse, severe pelvic pressure and other symptoms are common as fibroids get bigger and bigger.
Infertility is not very common in women with fibroids. It is often blamed for the infertility but usually it is associated with endometriosis or adenomyosis which is causing the infertility. HOWEVER, the check of the structure of the uterus is always made if a woman suffers recurrent miscarriages or long term infertility. Certainly it is know that those fibroids that impinge on the uterine cavity do cause fertility issues. These certainly need removal or embolisation.
Generally speaking, fibroids are NOT painful so that if a patient comes along with pain and diagnosis of fibroids on ultrasound scan, I always look elsewhere for the diagnosis.
DIAGNOSIS OF FIBROIDS
The following lists the various options available for diagnosis:
A simple vaginal examination, sometimes with a vaginal probe ultrasound examination (similar discomfort to a Pap smear) or an abdominal ultrasound examination with a very full bladder, are the main tools by which doctors diagnose fibroids. Modern ultrasound can detect fibroids as small as 1cm, or less, but it is more important to locate the site of the fibroid eg. fibroid lumps within the cavity or near the cavity of the uterus are the ones that are most often symptomatic.
An MRI scan (magnetic residence imaging) is very useful for diagnosing fibroids, but unfortunately is expensive and there is currently no Medicare rebate and probably it is not much more help than a simple ultrasound examination.
Sono historiography (vaginal ultrasound using sterile fluid inside the uterine cavity) is a newer way to locate intrauterine fibroids and polyps.
Hysteroscopy (using a small telescope to look inside the cavity of the uterus) is also simple and very useful way to diagnose fibroids
I did previously perform outpatient office hysteroscopies but found it unsuitable for private practice because of the extra staff required to be with the patient.

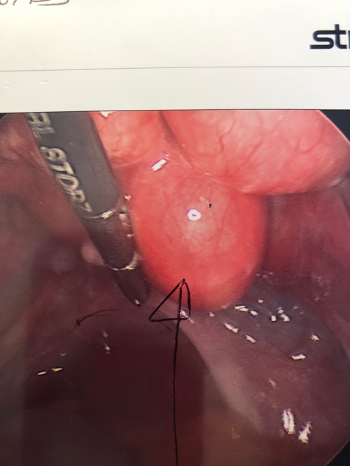
Picture of a 3cm submucous fibroid these fibroids protrude into the cavity of the uterus and are associated with very heavy periods
TREATMENT OPTIONS AVAILABLE FOR FIBROIDS
Often, now more than observation is necessary once the fibroid has been diagnosed. However, in cases where there are symptoms, either medical treatment or surgical treatment (minor or major) may be necessary. More recently, radiology has been used to treat fibroids as well.
Medical Options
The oral contraceptive pill usually does not increase the size of a fibroid and in some women may be sufficient to decrease heavy bleeding. This, however, is unlikely.
Secondly, women sometimes benefit from more powerful, although somewhat controversial drugs called GnRH agonists (controversy simply in their use for fibroids). The problem with the use of GnRH agonists (which are very successful in treating endometriosis and used commonly for IVF cycles) is that they sometimes produce dramatic and severe side effects, and unfortunately in most cases the fibroids can regrow, back to their original size in 4 to 6 months. Therefore, GnRH agonists are simply useful as an adjunct or aid to surgery (to shrink the fibroid down prior to its embolization or surgical removal.
Surgical Treatments for Uterine Fibroids
There are 5 main surgical options available to treat fibroids.
Myomectomy
Transcervical hysteroscopic resection (see picture 62)
Myolysis
Hysterectomy
Embolization (UFE)

A submucous fibroid that has been partly resected hysteroscopically
Firstly, myomectomy is a surgical procedure where the fibroid is removed via a major incision in the abdomen or laparoscopically through smaller incision. The choice will depend on the size, number, site of the fibroids and experience of the surgeon.
IRRESPECTIVE OF THE SURGICAL METHOD CHOSEN, THE FIBROIDS ARE REMOVED BUT THE UTERUS IS NOT
Hysteroscopic resection involves inserting an operating telescope into the uterus and shaving off pieces of the fibroid and removing them through the cervix. NB. This technique is not suitable for fibroids lying deep in the muscle of the uterus. This is a recipe for uterine perforation. It is most suitable for fibroids on a stalk, which are hanging into the uterine cavity. (see picture 62)
Myolysis is a somewhat controversial new surgical treatment involving insertion of a needle into the fibroid during laparoscopy. The needle cauterises the blood supply to the fibroid, thereby shrinking it over time. However, there is insufficient data to support its use in women who may wish to become pregnant later. (possible risk of uterine rupture in labour)
Although hysterectomy is the only true curative surgical treatment for fibroids, most women with fibroids will never need a hysterectomy! Despite this, about one third of all women will have a hysterectomy, and of these about one third will have a fibroid as a reason for the hysterectomy.
However, despite what the newspaper may say, most gynaecologists do not make women come in for unnecessary hysterectomies. After discussion with the gynaecologist, the patient chooses which treatment SHE would like, and she and her gynaecologist, after discussing the risks involved in each of the possible treatments, then adopt a plan of management, individualised for her particular needs.
Although hysterectomy is an important and often necessary treatment for fibroids, as with all major operations, the patient should be well aware of the possible risks and alternative treatments that do not require major pelvic surgery eg. hysteroscopic removal (above) and UFE (below).
A technique called UFE (uterine fibroid embolization) which has been available for other sites of the body for over 40 years and is called EMBOLIZATION. UFE involves the placing of a catheter (fine tube) into the blood vessel supplying the particular organ, in this case the uterus and then injecting a material along that catheter to block off the blood supply to the organ (uterus).
In the case of uterine fibroid it is not the whole organ that is blocked off, but just the intrauterine fibroid.
Conditions that Mimic Fibroids
There are several conditions that can mimic a fibroid and lead to difficulty in initial diagnosis.
Adenomyosis is a common condition found at the time of the removal of fibroids (usually diagnosed at hysterectomy) when the whole of the uterus is cut up, slices placed on a glass slide, stained and looked at under the microscope. However, more recently Adenomyosis has been able to be diagnosed by MRI scan and quality ultrasound devices. Adenomyosis is a condition where the endometrial lining (lining of the womb or uterus) eats through or grows into the muscle of the uterus. This disease therefore enlarges the uterus and causes the confusion in diagnosis, mainly by the subsequent increase in size of the uterus. The uterus full of adenomyosis is often described as bulky, but multiple small fibroids may also be bulky. Adenomyosis therefore can imitate fibroids, not only at the time of internal examination, but also at the time of ultrasound scan.
Uterine cancer is uncommon but must be excluded in women who have ABNORMAL UTERINE BLEEDING. If they have a uterine fibroid as well, one must not blame the fibroid until other causes of the bleeding had been excluded. Importantly, not all abnormal bleeding, associated with fibroids will be due to cancer, but it MUST be excluded, especially if a radiological treatment such as EMBOLIZATION is to be undertaken.
Ovarian cysts or lumps can mimic a fibroid. These can be dangerous because ovarian lumps have a much higher chance of being malignant (cancerous) than do fibroids. It is not uncommon for an inexperienced gynaecologist to be fooled into thinking that an ovarian lump is a fibroid and the possibility exists that the opportunity to treat an ovarian cancer early, may indeed be missed.
Treatment for fibroids
Treatment has been arranged here in increasing order of invasiveness)
Transcervical resection of fibroids – using an operating hysteroscope call a Resectoscope, can be done as a day surgery patient (you go home the same day) but is only and only suitable for submucous type fibroids (fibroids within the cavity of the uterus). A diagnosis of endometriosis should also be excluded at the time by doing a laparoscopy, if there has been pain. Generally speaking fibroids do not cause pain.
Radiological Fibroid Embolization – this procedure involves blocking up the blood vessels supplying the fibroid as outlined above. Can only be performed by an experienced interventional radiologist.
Myolysis – very similar, but more invasive than radiological fibroid embolization – involves the laparoscopic insertion of an electro-surgical wire to drill into the centre of the fibroid. Several drillings are needed for each fibroid. The recurrence rate is said to be high and is not commonly practice in Brisbane.
Laparoscopic myomectomy – the fibroid is shelled out by using keyhole surgery and the resultant hole or defect in the uterus is repaired. For large fibroids, difficulty can be encountered in retrieving the specimen. In order to cut the fibroid into pieces which can be removed, the procedure can sometimes be prolonged. With prolongation of the procedure there can be excess bleeding.
To repair the defect in the uterus laparoscopically is technically difficult. Because of this, care must be taken in selecting how big a fibroid one wishes to tackle in doing a laparoscopic myomectomy and indeed whether the fibroids really needs removal. It is probably not suitable for women who have not had children because of the major risk of uterine rupture at the point of the resultant scar, during the course of the pregnancy.
Laparoscopic myomectomy with colpotomy (creating an opening at the top of the vagina to retrieve the specimen (this has many of the same problems outlined in (4) above.
Laparoscopic mini laparotomy/myomectomy (laparoscopically assisted myomectomy (LAM) – the fibroid is shelled out laparoscopically but the defect in the uterus is repaired through a conventional (although much smaller incision in the abdomen. Patients can leave hospital much faster than conventional myomectomy.